
Bipolar disorder can be one of the most difficult disorders to diagnose. The reason is simple:
Half of bipolar disorder IS Major Depression.
That the other half is the presence or history of a manic episode presents a problem, and the problem is that most people don't come in to the clinic when they are in the throws of a manic episode. Why? Grandiosity. When most people experience a manic episode they feel pretty good about themselves. They have lots of energy, they feel like they are on top of the world, they're getting stuff done. What's not to like?
Then the plunge into depression, and come into the clinic telling us all about how depressed they are, which makes us think - of course - that they're depressed. Which they are. But that's not the diagnosis.
Good counselors will know to screen hard for any history of mania when they are hearing complaints of depression. But we can't read minds, so if the person minimizes the mania that they have experienced or don't report it at all, we are left to wait and see if any more manic episodes materialize through the course of treatment.
Here's the pharmacological trouble. If we think of bipolar as occuring on a scale, with feeling normal in the middle, the rollercoaster that is a patient suffering Bipolar might look something like this:
Half of bipolar disorder IS Major Depression.
That the other half is the presence or history of a manic episode presents a problem, and the problem is that most people don't come in to the clinic when they are in the throws of a manic episode. Why? Grandiosity. When most people experience a manic episode they feel pretty good about themselves. They have lots of energy, they feel like they are on top of the world, they're getting stuff done. What's not to like?
Then the plunge into depression, and come into the clinic telling us all about how depressed they are, which makes us think - of course - that they're depressed. Which they are. But that's not the diagnosis.
Good counselors will know to screen hard for any history of mania when they are hearing complaints of depression. But we can't read minds, so if the person minimizes the mania that they have experienced or don't report it at all, we are left to wait and see if any more manic episodes materialize through the course of treatment.
Here's the pharmacological trouble. If we think of bipolar as occuring on a scale, with feeling normal in the middle, the rollercoaster that is a patient suffering Bipolar might look something like this:
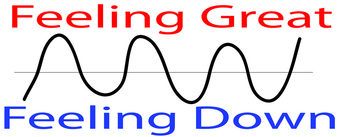
So we are likely to only see someone when they are on the bottom end of one of their cycles, because people generally don't like being depressed and it is at this point that they will seek help.
Now if we look at Major Depression moods on a graph, it might look something like this:
Now if we look at Major Depression moods on a graph, it might look something like this:
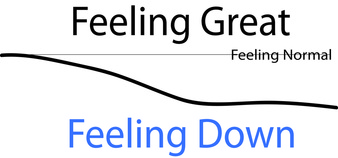
The trouble comes when we believe that someone is depressed, but they really have Bipolar, and we give them an antidepressant. Once the person begins their natural bipolar cycle into the wave of "feeling great" the antidepressant has a chance of kicking that into high gear and the person may become even more manic than usual. This can be very dangerous because the person is more likely to engage in risky behaviors that they might not ordinarily engage in, which could do significant harm to their lives.
So make sure that when you go in to see a clinician that you are giving as complete a history as possible. And remember that the common factor in any mental illness is a significant decline in functioning. So if you still have a job and your family still wants you to come around and you are still bathing and leaving the house, a psychiatric diagnosis may not be warranted. But if their are significant disruptions in life and you suspect a mental illness may be the cause, the best thing to do is to consult a mental health practitioner as soon as possible
So make sure that when you go in to see a clinician that you are giving as complete a history as possible. And remember that the common factor in any mental illness is a significant decline in functioning. So if you still have a job and your family still wants you to come around and you are still bathing and leaving the house, a psychiatric diagnosis may not be warranted. But if their are significant disruptions in life and you suspect a mental illness may be the cause, the best thing to do is to consult a mental health practitioner as soon as possible
Chase Chick MPA LPC is CEO and co-founder of Beyond the Gray Sky, whose brands include Pursuit of Happiness, Dallas Psychology Review, and Luxe Media Productions.
 RSS Feed
RSS Feed
